Augmentative and Alternative Communication in Early Intervention

Augmentative and alternative communication (AAC) can play a crucial role in supporting early language development and communication skills in early intervention (EI). Speech-language pathologists (SLPs) play a critical role in introducing and supporting AAC, empowering families, and ensuring that every child has access to effective communication with their caregivers.
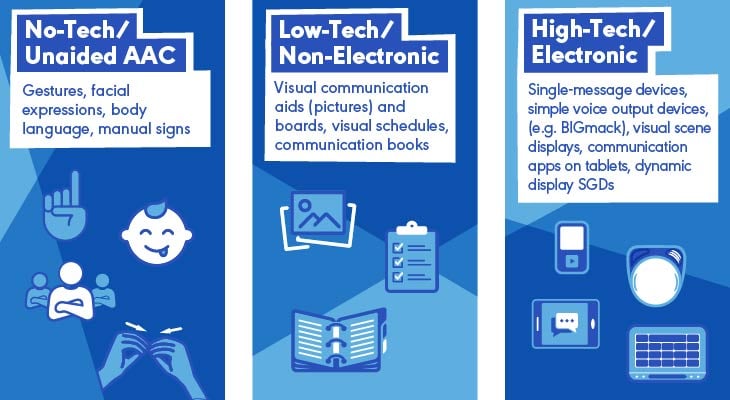
AAC includes all forms of communication other than spoken language that support or replace verbal communication. AAC ranges from low-tech options—such as gestures, signs, and picture boards—to high-tech speech-generating devices (SGDs) and apps. AAC can be used temporarily or as a long-term communication support.
There are no prerequisites for considering or introducing AAC, including doing so in work with young children.
The information below is specific to supporting SLPs who provide services to the birth-to-three population. It is meant to be a simple guide to support your success as an EI provider.
For a broader overview of AAC, please visit ASHA’s Practice Portal page, Augmentative and Alternative Communication (AAC).
Principles of AAC in EI
SLPs are the most qualified service providers—based on their training and education—to assess the need for AAC and to implement AAC strategies with toddlers. Their understanding of early symbolic language development, cognitive–linguistic milestones, and communication intent enables them to design and introduce functional AAC systems tailored to young children’s needs. SLPs can initiate AAC supports and also complete a comprehensive SGD evaluation, particularly when a child’s needs go beyond what can be addressed with low-tech or interim solutions.
Common Facts About AAC in Early Intervention
AAC can and should be introduced early to support language development.
Research shows that AAC supports verbal language development.
All children can learn to communicate with AAC—with personalized supports.
Any child with communication challenges can benefit from AAC.
Caregiver Education
Educating caregivers and communication partners about AAC is essential to creating consistent, responsive communication environments for young children. This section offers clear, family-friendly information to dispel common myths and explain how AAC supports early language development. When caregivers understand the purpose and potential of AAC, they are better equipped to integrate it into daily routines and create meaningful opportunities for their child to communicate.
Essential Insights—What Families Should Know About AAC
AAC Is Appropriate for Infants and Toddlers
- There is no “too young” of an age for AAC. Early exposure to multimodal communication supports language and cognitive development.
- AAC should be introduced as soon as a child demonstrates difficulty developing spoken communication.
- AAC is not the same as “screen time.” Although AAC apps are used on electronic devices, the child is actively using the technology to communicate their thoughts and needs.
AAC Does Not Hinder Speech Development
Research shows that AAC supports and even increases spoken language development in young children.
- Early Intervention and AAC: What a Difference 30 Years Makes: This systematic review linked from ASHA’s Evidence Maps states, “The evidence strongly indicates that [augmentative and alternative communication] AAC does not hinder the development of speech at the very beginning stages of language acquisition” (p. 194).
- Impact of Speech Generating Device Interventions on Vocalizations of Individuals With Autism and Severe Communication Impairment: A Systematic Review of the Research (from ASHA’s Evidence Maps) shared that 87% of the participants across studies demonstrated improvement in vocal utterances—with no studies reporting a decrease in spoken language when speech-generating devices were part of the intervention.
- Prescribing Assistive Technology: Focus on Children With Complex Communication Needs (from the American Academy of Pediatrics [AAP]) includes additional information that can be shared with pediatricians to support the need for AAC for early communication development.
- AAC With Energy—Earlier: This article from The ASHA Leader offers a research summary of AAC use in young children introduced to augmentative and alternative communication as early as 12 months.
When paired with verbal modeling, AAC can encourage spoken communication rather than replace it.
Presume Potential, and Support Language Growth
- Young children benefit from rich language exposure, just like their typically developing peers.
- Young children who use AAC can learn to use single, descriptive words and picture supports to assist with helping them ask for what they want, refuse what they don’t want, get someone’s attention, or comment on favorite topics.
Family and Caregiver Coaching Is Essential
- Training families and communication partners on AAC use in natural routines (e.g., mealtime, play, bath time) encourages communication opportunities throughout the day.
- Learning any skill takes practice. Practicing communicating with AAC in all environments can support vocabulary development all day long.
SLPs who work in EI can show caregivers how to include AAC and consult with other therapists on the individualized family services plan (IFSP) team to get everyone involved!
Access to AAC Should Be Consistent and Functional
- AAC should always be available, just like spoken language.
- Communication partners can integrate chosen systems into the child’s daily environment and routines.
Resources Related to Early and Person-Centered AAC Options
- AAC and Families: Dispelling Myths and Empowering Parents
- The ASHA Leader article, From Frustration to Understanding: An AAC Story of Presuming Potential, highlights the principle behind presuming potential.
- The ASHA Voices podcast, Why Some Autistic People Choose AAC and Oral Speech, talks about how people should have better access to AAC and that it should be treated on level with any other communication form—not just as a last resort. This is a consideration across the lifespan.
- Beyond Spoken Words: Augmentative and Alternative Communication (AAC) from the American Academy of Pediatrics offers information about AAC to educate parents and caregivers.
- Exploring core competencies for language facilitation in parent training programs in AAC: Disability and Rehabilitation includes supplemental materials and charts that share training resources in both English and Spanish to support caregiver training on topics such as modeling, prompting, caregiver feedback, environmental modifications, responsivity, wait time, and expectant delay.
Assistive Technology
Assistive technology (AT) refers to any item, equipment, or system that enhances functional capabilities for individuals with disabilities. AAC is a type of AT that focuses specifically on supporting communication. It includes a range of tools—from no-tech strategies to advanced SGDs—designed to facilitate communication.
AT can include tools like proximity switches, mounting systems for adaptive chairs, and head mounts or eye-gaze tracking for children with motor impairments.
The right AT setup ensures that the child can effectively access and use AAC.
Types of AAC To Consider
Selected Resources
- See ECTA Center: Assistive Technology for a description of evaluation guidance.
- See the Center on Technology and Disability (a program of the Assistive Technology Center) for free resources, webinars, articles, guides, and training materials related to providing high-quality education to children with disabilities.
Assessment and AAC Selection in Early Intervention
Evaluating a child’s need for AAC and implementing appropriate support is well within the Scope of Practice in Speech-Language Pathology. Specialized certification is not required to begin this process—SLPs are trained to identify communication needs, trial AAC strategies, and support early implementation. SLPs can participate in training to learn more about assessing and supporting AAC, and many free or low-cost resources are available that can help. When a child presents with complex access needs or when more in-depth feature matching is required, SLPs can collaborate with colleagues or AT specialists to ensure comprehensive support. The key is to begin early and work as a team to provide the child with a functional means of communication.
Dynamic and Play-Based Assessment
|
Trialing AAC Options
|
Multimodal Communication Assessment TemplateThis template [PDF] is designed to guide SLPs through the process of assessing multimodal communication needs in EI. It supports a collaborative, play-based approach that considers each child’s unique strengths, interests, and challenges. The template helps SLPs document key observations, trial AAC options, and plan individualized strategies that align with family routines and developmental goals over one or even multiple sessions. Information from the data will be useful if the SLP is referring for a funded SGD evaluation. Use it as a practical tool for organizing information, facilitating team collaboration, and planning next steps in multimodal communication and AAC implementation. |
To learn more about funding considerations for AAC devices, please visit ASHA’s Practice Portal page on Augmentative and Alternative Communication (AAC), and scroll to the section on “Reimbursement and Funding. |
Implementation Strategies
Introducing AAC in EI is most effective when it’s embedded naturally into a child’s everyday life. This section offers practical, family-friendly strategies to help SLPs and caregivers build communication opportunities into daily routines and make AAC engaging and meaningful. Through consistent modeling, simple tools, and playful interaction, young children can begin to understand and use AAC as a functional part of how they connect with others.
Customization and Personalization
|
Model AAC Use (“Aided Language Stimulation”)
Example: During snack time, a caregiver can point to the “eat” symbol on the child’s AAC system while saying, “Let’s eat?” This simple pairing of speech with symbols helps the child associate the words with both their meaning and visual representation. Coach the caregiver by modeling the use of AAC and spoken language during snack time, then guiding them through practice. Example: Place a real photo of the child’s favorite toy (e.g., stacking blocks) directly under the child’s stacking blocks for them to discover when they lift the block. This can be an introductory step as they begin to associate pictures with real items. Coach the parent to point to the photo and talk about the stacking blocks as the child begins to play with them. |
Embed AAC in Everyday Routines
Example: Print pictures for a paper communication board with familiar items, places, and activities. At daycare, have simple pictures of shoes and a picture of the child’s parent or caregiver available, and use them for transitioning home. Coach the daycare provider to model AAC use (e.g., “Let’s get your [SHOES] so we can go to mom” while pointing to the pictures of [SHOES] and of [MOM]”) |
Keep It Simple and Engaging
Example: When singing a song with the child, model a symbol paired with a word during the song (e.g., “Wash, wash, wash your hands”). Repetition in a song reinforces learning of new vocabulary and engages the child’s attention. The communication partner can imitate the action of washing and then point to an image of hands. The activity can be incorporated into play, pretending to wash stuffed toys while modeling AAC use by pointing to pictures of different body parts to wash, all while singing a fun tune. |
Support Social Interaction
Example: Introducing a single recordable button can be fun and engaging for the child. You can record a single core word—such as “Go”—and model activating the button while using the verbal routine, “Ready, set, (press button “go”) and proceed with play. Coach the caregiver to continue to support the child by modeling and moving the button so the child can continue to engage. You can add on to the activity—or scaffold—by adding another communication partner. Coach another caregiver or sibling to activate a “stop” recordable button when the toy stops moving. |
|
Case Studies: AAC in Early Intervention
Case studies can provide practical examples of how AAC is introduced and implemented across a range of developmental profiles. The following scenarios illustrate how SLPs can use their clinical judgment to assess communication needs, select appropriate AAC supports, and partner with families to embed AAC into everyday routines. Each case highlights different considerations to support confident, informed decision making in EI.
Background
Child: Emma, 22 months old
Diagnosis: Global developmental delays
Setting: Home-based EI services due to delays in gross motor, fine motor, and expressive language skills
Family Concerns: Emma primarily used gestures (e.g., pointing, waving) and a few spoken word approximations (e.g., “ba” for bottle). She would become frustrated when unable to express herself, leading to meltdowns.
To support Emma’s communication skills, the SLP recommended a multimodal approach, which required a multimodal communication assessment.
Assessment and Initial AAC Trial
The SLP conducted a play-based AAC assessment focusing on Emma’s receptive language, motor abilities, and communication attempts. Observations included the following:
- strong understanding of familiar words and simple commands
- frequent pointing with fist, reaching, and vocalizations when engaging with toys and family members
- emerging interest in picture books and cause-and-effect toys
- limited verbal imitation but consistent nonverbal communication
Based on these findings, the SLP recommended a multimodal AAC approach incorporating gestures, signs, a low-tech picture communication board, and trialing a speech-generating AAC app on a tablet.
Implementation Plan
Phase 1: Introducing AAC
-
Aided Language Stimulation: The SLP modeled using the picture communication board and AAC app during play and daily routines, such as snack time.
-
Core Vocabulary Focus: The initial words chosen were high-frequency, functional words like more, help, go, stop, and all done.
-
Family Training: The SLP coached parents on using AAC during routines, such as modeling “more” on the board when Emma reached for a snack.
-
Encouraging Engagement: The SLP incorporated the AAC system into preferred activities (e.g., music time, playing with bubbles) to build motivation.
Phase 2: Expanding Use
-
Emma began independently selecting symbols for more and go to request favorite activities when safely secured in her highchair. The communication partners increased toy or food options and modeled pointing to the object paired with modeling “mas” on a recordable switch and verbalizing “mas.”
-
Parents reported a decrease in frustration behaviors as Emma gained a way to express needs and gain attention from caregivers using a recordable button.
-
The SLP introduced additional words—including social phrases like hi and bye—to support interaction.
-
The SLP added things to the AAC system, integrating more personalized symbols (e.g., Emma’s favorite toys and foods) and incorporating a recordable mid-tech device with additional buttons.
Phase 3: Generalization and Speech Support
-
Emma consistently used AAC at home and during play dates.
-
Verbal approximations increased alongside AAC use, with Emma attempting words like “muh” for more/mas and “go” while using the AAC system.
-
Emma’s parents became more confident in modeling AAC, gestures, and spoken words and embedding them naturally into their routines.
-
The SLP collaborated with Emma’s occupational therapist to explore switch-access technology for future AAC access, considering fine-motor challenges.
Outcome
Through a carefully implemented multimodal AAC approach, Emma developed a reliable means to communicate her needs and participate more fully in daily routines. Her independent use of AAC symbols reduced frustration and meltdowns, and her increased verbal approximations reflected progress in spoken language development. Family involvement and coaching were key factors in embedding AAC naturally at home, fostering consistent use and supporting Emma’s overall communication growth. Collaboration with the occupational therapist further ensured that future AAC access options would meet Emma’s evolving motor abilities, promoting continued success. Using the information gathered in the multimodal communication assessment, progress reports, and parent input, Emma was referred for a comprehensive AAC evaluation to obtain a dedicated speech-generating device (SGD).
Background
Child: Noah, 26 months old
Diagnosis: Cerebral palsy (spastic quadriplegia), cortical visual impairment (CVI), significant receptive and expressive language delays
Setting: Home-based EI services as part of an interdisciplinary team
Family Concerns: Noah was not using spoken language and had limited ways to express wants or needs. His parents reported frequent feelings of frustration during daily routines and a desire to better understand what he wanted. Motor and visual impairments seemed to be impacting communication development.
To support Noah’s ability to communicate, the SLP initiated a referral to an assistive technology (AT) specialist for a comprehensive AT evaluation in collaboration with his EI team—which included an occupational therapist, a physical therapist, and a teacher of children with visual impairments.
Assessment and Initial AAC Trial
The AT specialist used a collaborative, routines-based assessment approach that considered Noah’s sensory and motor profiles as well as his communication behaviors. Observations included the following:
- consistent responses to voices and familiar sounds
- limited hand use, with some controlled movement in his right thumb and index finger
- strong interest in preferred objects with high-contrast colors
- communicative intent through vocalizations, body movements, and changes in facial expression
The SLP presented information about familiar symbols and vocabulary that Noah had been working on using data gathered from their AAC assessment. With input from the occupational therapist and a vision specialist, the team trialed a combination of tactile symbols, auditory scanning with an SGD, and a single-switch system for access. The SLP completed a comprehensive AAC evaluation, and Noah received his funded AAC device.
Implementation Plan
Phase 1: Building Access and Familiarity
-
Customized Access: The AT specialist recommended mounting the SGD on a stable surface near Noah’s adaptive chair and positioned a single pressure- activated switch near Noah’s right elbow.
-
Partner-Assisted Scanning: The SLP and family practiced partner-assisted auditory scanning using simple choices (e.g., “Look! Let’s play! Music [pause] Book [pause]”). The caregiver responded to Noah’s gaze and vocal cues (“Oh! Book! I see you are looking at the book. Let’s read the book!”)
-
Family Training: The team trained Noah’s caregivers to recognize and respond to Noah’s nonverbal signals for “yes” and “no.” They modeled consistent language input and paired spoken words with AAC output using switch activation to indicate “yes.”
-
Motivation-Driven Content: The SGD was initially paired with meaningful activities, such as playing with musical toys and listening to family members’ voices. The family used portable recordable switches for other activities to practice and encourage AAC in all daily routines using personalized vocabulary.
Phase 2: Expanding Functional Communication
-
Noah began using the switch to indicate preferred choices during mealtime and play.
-
The family noticed a reduction in frustration and greater anticipation during routines where he could participate using his AAC system.
-
Noah expanded his vocabulary to include greetings, choices, and basic needs like “more,” “stop,” “yes,” and “all done.”
Phase 3: Promoting Interaction and Participation
-
Noah used his SGD to greet his siblings, request music, and signal “all done” during therapy sessions.
-
The SLP collaborated with the occupational therapist and the AT specialist to optimize switch placement. The SLP also collaborated with the vision specialist to improve symbol clarity using CVI strategies (e.g., use of red/yellow icons, reduction of visual clutter).
-
His parents became more confident integrating AAC into everyday routines and advocating for access in other environments.
Outcome
With a tailored AAC system that considered his complex motor and sensory needs, Noah gained a consistent way to communicate. His increased engagement and reduced frustration improved the overall quality of family interactions. The case illustrates how early AAC intervention, in collaboration with an interdisciplinary team, can empower children with complex needs to participate meaningfully in daily life.
Background
Child: Leo, 24 months old
Diagnosis: Autism spectrum disorder (ASD), language delay
Setting: Home-based EI services with parent coaching
Family Concerns: Leo communicated primarily through gestures, pulling adults toward desired items and occasionally screaming or crying when he was misunderstood. He had not yet developed spoken words and preferred to play alone. His parents wanted to support his communication but were unsure how to begin.
The SLP recommended an AAC assessment to explore ways to support functional communication, reduce frustration, and encourage joint engagement.
Assessment and Initial AAC Trial
The SLP used a play-based assessment with caregiver input and observation during familiar routines. Observations included the following:
- strong visual attention to objects of interest (e.g., favorite snacks, tablet, toy trains)
- limited response to his name but emerging interest in predictable routines (e.g., snack time, bath time)
- communicative intent observed through reaching, eye gaze, and pulling caregivers toward desired items
- no observed joint attention with communication partners
- increased agitation when communication partners attempt to engage in parallel play
- abandoning of activity when communication partner joins play
Based on Leo’s strengths and interests, the SLP introduced a low-tech picture communication board with core vocabulary and trialed a speech-generating AAC app with visual supports and voice output.
Implementation Plan
Phase 1: Introducing AAC Through Routines
-
Aided Language Stimulation: The SLP modeled using the communication board and AAC app during predictable routines like snack and play times.
-
Motivating Vocabulary: Initial symbols included highly preferred items like “cracker,” “go,” “tablet,” and “music” as well as social words like “more” and “all done.”
-
Parent Coaching: The SLP coached Leo’s parents on how to pause, model AAC use, and respond consistently to Leo’s communicative attempts using AAC.
-
Embedding in Play: The SLP introduced AAC during Leo’s favorite activity—rolling trains—to model words like “go,” “stop,” and “more.”
Phase 2: Increasing Engagement and Symbol Use
-
Leo began using the AAC app to request preferred snacks and toys with prompts and modeling.
-
Leo’s parents reported a decrease in his meltdowns and an increase in his successful communication attempts.
-
Leo expanded his vocabulary to include action words (e.g., open, eat), people’s names, and early social words (e.g., hi, bye).
-
The SLP and Leo’s family personalized the AAC app with familiar photos and audio to increase engagement.
Phase 3: Supporting Interaction and Language Growth
-
Leo initiated more interactions using his AAC system, especially during snack and music routines.
-
Leo’s parents became more responsive to Leo’s nonverbal communication attempts, using the AAC system to model new words during shared activities.
-
Verbal approximations emerged alongside AAC use, such as “ba” for ball and “ma” for more.
-
The SLP continued coaching his parents to follow Leo’s lead, model AAC naturally, and reinforce all communication attempts.
Outcome
Leo began using his AAC system to make choices, participate in daily routines, and reduce frustration. His parents gained confidence using AAC strategies and reported stronger connections with Leo through shared communication experiences. This case demonstrates how AAC can be a powerful early support for autistic toddlers—enhancing communication, building interaction, and supporting multimodal language development.










