Early Hearing Detection and Intervention

Early Hearing Detection and Intervention or “EHDI” refers to the nationwide effort to identify hearing loss in newborns and infants as early as possible and provide timely intervention. Between 1 and 2 out of every 1,000 newborns in the U.S. are identified as deaf or hard of hearing. Without timely support, these children face risks of developmental, social and cognitive delays. The goal of EHDI is to ensure that children who are born deaf or hard of hearing receive appropriate support and services to optimize their communication skills and overall development.
Key components of EHDI programs typically include the following:
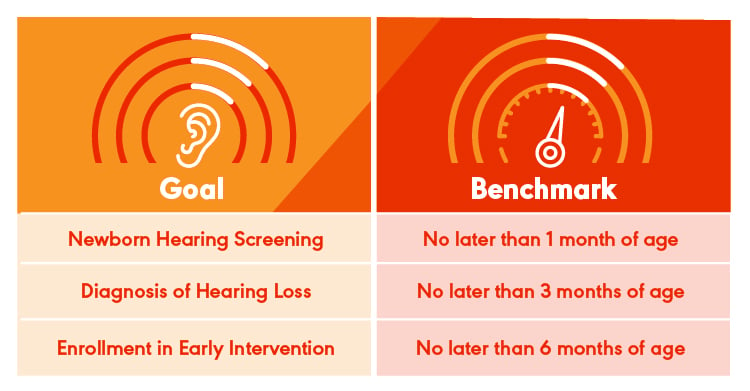
- Newborn Hearing Screening: Newborns are screened for hearing loss—usually before leaving the hospital.
- Identification: If a child does not pass their newborn hearing screening, then an audiologist conducts a comprehensive audiological evaluation to determine the type, degree, and configuration of hearing levels in each ear.
- Intervention: Once an audiologist diagnoses hearing loss, they implement or refer to appropriate interventions, which might include hearing devices (e.g., hearing aids or cochlear implants), services such as speech and language therapy, and family-to-family support programs.
- Follow-Up: It is critical that the child receives ongoing monitoring and programming of hearing technology and communication development.
1-3-6 Benchmarks
In 2000, the Joint Commission on Infant Hearing (JCIH) established specific guidelines [PDF] to ensure that newborns and infants who are deaf and hard of hearing are identified and receive appropriate interventions in a timely manner. These benchmarks help measure the effectiveness and efficiency of EHDI programs.
How EHDI Is Funded
EHDI programs are funded through a shared cost model. It is a combination of federal, state, and local funding—as well as private sources. The specific funding mechanisms vary depending on the state and health care system in place, but generally speaking, the funding for EHDI comes from three main sources:
U.S. Federal FundingCenters for Disease Control and Prevention (CDC): The CDC provides federal grants to some U.S. states to support their EHDI programs. These grants are designed to aid state programs in collecting and analyzing data. Data analysis can provide states with ideas on how to improve their EHDI programs. CDC data provides critical EHDI information such as (a) how well each state is doing to meet 1-3-6 benchmarks (b) how well the country is doing to meet the 1-3-6 benchmarks and (c) the prevalence of hearing loss in infancy. Health Resources and Services Administration (HRSA): HRSA is another federal agency that provides funding that is specifically aimed at supporting the development and improvement of EHDI systems. In 2024, HRSA awarded grants to 59 states and territories. HRSA also funds the EHDI National Network—which includes the Implementation and Change Center (ICC), Provider Education Center (PEC), and Family Leadership in Language and Learning Center (FL3). |
State FundingMedicaid: Medicaid can cover various services related to hearing loss, including hearing screenings, diagnostic testing, hearing aids, cochlear implants, speech therapy, and early intervention services. Medicaid is a joint federal and state program, and its coverage varies by state. State-determined funding: Many states have their own funding mechanisms and programs to support EHDI services. State health departments may allocate state funds to assist with newborn hearing screening, follow-up diagnosis, and early intervention services. Some states have specific state-level grants that further support EHDI activities, ensuring that local health departments and hospitals can conduct screenings and provide follow-up services. |
Private Health InsurancePrivate health insurance may cover some or all the costs related to hearing screenings, diagnostic testing, and treatments for hearing loss, such as hearing aids or cochlear implants. The specifics of coverage often depend on the health insurance policy and the type of hearing loss. |
Grants and Philanthropic FundingPhilanthropic organizations and individual donors may also provide funding to support EHDI efforts. For example, grants may be awarded to specific programs that aim to increase access to hearing screening and ensure that children with hearing loss receive early intervention services. Some programs may be designed to support low-income families or underserved populations, ensuring equitable access to services. |
The EHDI National Network
The EHDI National Network is federally funded through HRSA. It provides support for EHDI programs at the national, state, territory, and local levels and is divided into three centers:
- Implementation and Change Center (ICC)
The ICC helps state and territory EHDI programs implement evidence-based practices to support deaf and hard of hearing children and their families. The ICC aims to ensure that deaf and hard of hearing children receive quality services to meet their language milestones. A cooperative agreement with the Beacon Center at Gallaudet University supports the ICC. - Family Leadership in Language and Learning Center (FL3)
The FL3 works to strengthen family engagement, leadership, and family support across EHDI systems. A cooperative agreement with Hands & Voices supports the FL3 Center. - Provider Education Center (PEC)
The PEC helps health care professionals who screen, diagnose, and provide services to infants, children, and families interact with the EHDI system. A cooperative agreement with the American Academy of Pediatrics supports the PEC. ASHA is a sub-grantee to the EHDI PEC.
The LEND Program
LEND stands for Leadership Education in Neurodevelopmental and Related Disabilities. It’s a federally funded initiative that trains professionals to provide high-quality care to individuals with neurodevelopmental disabilities—such as autism, cerebral palsy, intellectual disabilities, and other related conditions like hearing loss.
The LEND program emphasizes interdisciplinary training and promotes leadership development in the field of disability services. It involves various disciplines like medicine, psychology, social work, nursing, public health, education, audiology, and speech-language pathology. Professionals who have been trained in this program are expected to improve service delivery, research, and policy advocacy for individuals with neurodevelopmental disabilities.
LEND Program's Pediatric Emphasis
The Pediatric Audiology Supplement in the LEND program is a specialized component that focuses on the role of audiology in the diagnosis, treatment, and support of individuals with neurodevelopmental disabilities. Audiologists are trained to work within multidisciplinary teams to assess and address hearing and communication issues in children with developmental disabilities. The supplement is designed to provide audiology professionals with specific training in how neurodevelopmental disabilities can affect auditory processing, speech, and language development. It often includes hands-on experience and collaboration with other professionals, ensuring that audiologists can contribute effectively to comprehensive care plans for these individuals. The United States has 52 LEND programs and 12 LEND Pediatric Audiology Supplement programs.
The Role of Audiologists in the EHDI System
Audiologists are essential to ensuring that children who are deaf and hard of hearing are identified early, receive appropriate diagnoses, and are connected to proper intervention services. Audiologists bring specialized knowledge of hearing and auditory processing to the multidisciplinary team. They work with families, health care providers, and other specialists to support optimal outcomes for children with hearing loss.
Here is a breakdown of the key roles that audiologists play in the EHDI system:
Audiologists are often involved in the design and implementation of newborn hearing screening programs. They help set up protocols for screening in hospitals and birth centers and may participate in the training of screeners to ensure that all babies are screened for hearing loss shortly after birth. Some audiologists also conduct newborn hearing screenings themselves.
Audiologists perform a full diagnostic assessment after a referral from the newborn hearing screening. This assessment includes conducting various tests such as otoacoustic emissions (OAEs), auditory brainstem response (ABR), pure-tone audiometry, and impedance testing. The type of test selected depends on the child’s history and age. These evaluations help determine the type, degree, and configuration of hearing loss (e.g., conductive, sensorineural, or mixed) and guide the intervention decisions. It is imperative that the audiologists who see infants and toddlers are trained to perform these specialty evaluations for the youngest pediatric population. If the audiologist does not feel comfortable performing these tests, then they should make a referral to an audiologist who is well versed in seeing pediatric patients to ensure the best quality of care.
The audiologist interprets diagnostic results and works with other health care providers to establish the child’s needs. This work can include identifying whether the hearing loss is permanent or fluctuating, whether the child might benefit from hearing aids or cochlear implants, and whether the child needs medical treatment.
Based on diagnostic findings, the audiologist often works alongside other professionals—pediatricians, otolaryngologists (also called ear/nose/throat doctors, or ENTs), family-to-family support specialists, early interventionists, and others—to further assess the child’s medical and developmental needs. Then, they make their referrals accordingly.
Audiologists help select and fit hearing aids, cochlear implants, and other assistive listening devices based on the child’s type and degree of hearing loss. They provide detailed guidance to families on how to use and care for these devices. For children with severe-to-profound hearing loss, audiologists assess whether the child is a candidate for cochlear implantation.
Audiologists help parents and caregivers understand the nature of their child’s hearing loss, including what the diagnosis means for their child’s development and communication.
Audiologists introduce families to the continuum of communication opportunities that are available: from listening and spoken language to sign language. Audiologists provide resources and support that align with family values, goals, and culture.
After a child is fitted with a hearing device, the audiologist provides regular follow-up care—approximately every 3 months—to monitor the effectiveness of the devices, check for any changes in hearing levels, and adjust the devices as the child’s needs evolve. Apart from adjusting the hearing device, the audiologist also makes sure that the earmolds used with the hearing aids are still an appropriate size. Children grow quickly—and so do their ears! So, making sure that their earmolds continue to fit well makes a big difference for the quality of sound that the hearing device provides.
The audiologist monitors the child’s auditory milestones over time to ensure that the hearing aids or implants still meet the child’s needs.
Audiologists may also be involved in training and supporting other professionals in the EHDI systems such as newborn hearing screeners, educators, social workers, and health care providers—to ensure that they understand the needs of children with hearing loss.
The Role of SLPs in the EHDI System
SLPs are an integral part of the EHDI system. Here are some key roles that they may play:
While SLPs are not typically the ones conducting newborn hearing screenings, they play a critical role in the follow-up process when a child does not pass the screening. They may be involved in referring the child to an audiologist or a specialist for further evaluation. SLPs who are involved in early intervention may also be the first provider to notice that a child may not be meeting developmental milestones and/or express concerns about the child’s responses to sound. Even a baby who passes their newborn hearing screening can develop hearing loss later in early childhood. When an SLP notices signs of hearing loss, a referral for a follow-up hearing screening is imperative. The SLP may also do a hearing screening as part of their evaluation process—and if a child does not pass the hearing screening, then the SLP can refer the child for a diagnostic evaluation by an audiologist. To find a pediatric audiologist in your area, refer to the Early Hearing Detection and Intervention Pediatric Audiology Links to Service (EHDI PALS) directory.
SLPs assess children who have been diagnosed with hearing loss or who show signs of communication delays. Assessing an infant or a toddler means using observation, interview, and criterion-referenced assessments to look at speech, language, and social communication as well as overall development. SLPs in early intervention collaborate with audiologists and other providers to connect assessment results with communication access.
Once a hearing loss is confirmed, SLPs play a key role in developing and implementing an individualized treatment plan for the child. This often involves any or all of the following:
-
Language development: Helping children develop language skills (both spoken and/or sign language) depending on the family’s goals and the child’s needs.
-
Speech therapy: Supporting speech development, production, and intelligibility.
-
Monitoring of hearing aids’ or cochlear implants’ effectiveness: As part of their role in supporting children in the use of their hearing devices, sometimes SLPs may conduct listening checks to make sure that the devices are working properly. SLPs may also note certain sounds that a child is having difficulty with and can share their findings with the child’s audiologist, who can make certain adjustments to give the child the best access to sound. It is important for SLPs who work in early intervention with young children who are deaf or hard of hearing to have working knowledge of hearing technology and troubleshooting. SLPs should understand that there is a link between (a) the child’s development and productions and (b) the child’s acoustic access.
-
Family education and support: Educating and coaching families on how to support their child’s language development at home, including ways to (a) embed language and communication throughout daily routines as well as (b) foster and optimize listening environments.
-
Monitoring of progress: SLPs regularly monitor the child’s progress and adjust therapy plans as needed. They record language milestones and communicate with other team members to ensure that the child’s development is on track.
-
Collaboration with the EHDI Team: SLPs work as part of a multidisciplinary team, collaborating with audiologists, pediatricians, early interventionists, and educators to provide a holistic approach to the child’s development. They participate in team meetings, share insights, and contribute to the development of comprehensive care plans.
Types of EHDI Policy
Federal Policy: On December 22, 2022, President Biden signed the Early Hearing Detection and Intervention (EHDI) Act of 2022 (S.4052) to be administered by the U.S. Department of Health and Human Services (HHS). The law amends the Public Health Service Act to reauthorize the EHDI program until Fiscal Year 2027. The law directs three HHS agencies—the Health Resources and Services Administration (HRSA), the Centers for Disease Control and Prevention (CDC), and the National Institutes of Health (NIH)—to continue coordinating and advancing a national program for the early identification and diagnosis of deaf or hard-of-hearing newborns and infants. Although S.4052 is authorized until the end of Fiscal Year 2027, the amount of funding authorized is determined yearly. ASHA staff and members work closely with partners on Capitol Hill to advocate for full funding annually.
State Policy: Each state has the option to enact legislation or provisions related to EHDI. NCHAM provides a summary of state laws and provisions related to newborn hearing screening. When young children are candidates for hearing aids, well-fit hearing aids are a key part in early intervention for hearing loss. Despite research clearly showing the benefit of properly fit hearing aids and language development, not all states cover hearing aids for children. NCHAM provides a summary of states that have enacted hearing aid legislation.
Hearing Screenings in Early Intervention
Between the newborn hearing screening and age 4, there are no required hearing screening recommendations except for children with risk factors. Early intervention programs vary greatly in the requirement or recommendation for hearing screening. A study published in 2024 showed that the prevalence of permanent hearing loss in childhood that is identified after the newborn hearing screening is at least as high as the number of children identified through newborn hearing screening. When slight, mild, and unilateral types of hearing loss are included, the prevalence is much higher.
Early intervention providers should consider incorporating hearing screenings. Audiologists and SLPs in early intervention should advocate for this screening to be added to early intervention evaluation protocol.
EHDI Data and Funding Trackers
The following resources provide and track EHDI data and funding:
- From the CDC: Annual Summary Data: Early Hearing Detection and Intervention (EHDI) Program
- From HRSA: Strengthening Early Hearing Detection and Intervention (EHDI)
EHDI Modifiable PowerPoint
This PowerPoint [PPT] was created for members to use when giving educational talks to other providers or the community about the role of audiologists and SLPs in the EHDI system. Incorporate your photos, clinic or school district logo, and add slides.










